






Most of us have probably experienced shoulder pain at some point, something pretty common in gym rooms
Index
- 1 Shoulder joint and scapula
- 2 How to spot problems with the scapulas?
- 3 Shoulder correction and rehabilitation
- 4 Shoulder Impingement
- 5
- 6 Causes of Shoulder Impingement
- 7
- 8 Stages of impingement injury
- 9
- 10 Symptoms of Shoulder Impingement
- 11 Treatment and rehab exercises for shoulder impingement
- 12
- 13 Videos to treat Shoulder Pain
- 14 Recommendations
- 15 Sources
- 16 Related Posts
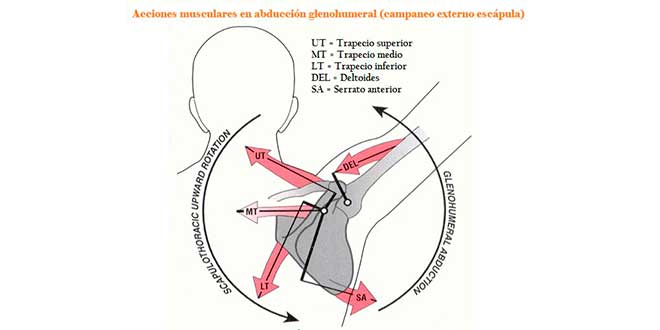
Shoulder joint and scapula
The main function of the scapula is to keep the shoulder joint stable during movement by connecting it to the rest of the trunk. So, a coordinated movement rhythm of the scapula relative to the glenohumeral joint during exercise gives the humerus a mechanical advantage or disadvantage.
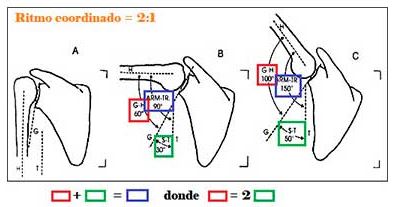
The optimal scapulohumeral rhythm is the one that allows for every 15º of movement in the joint complex, 10º come from the glenohumeral joint and 5º from scapular rotation (image below).
When there’s a dynamic and/or static alteration of this rhythm, it’s considered scapular dyskinesis
How to spot problems with the scapulas?
Presence of bony prominences on any of the edges or angles of the scapula
Scapular Retraction Test (SRT) – assesses rhomboid strength
Perform a bilateral scapular retraction and hold an isometric contraction for about 10 – 15 seconds. The inability to maintain a sustained contraction, accompanied by pain or burning in the rhomboid area, suggests dyskinesis in one of the two scapulas 
Shoulder flexion without weight VS shoulder flexion with weight
The image on the right shows a noticeable increase in scapular dyskinesis, although you could spot something in the left image when raising the arm without weight. The prominence of the superior medial angle of the scapula in the left photo indicates some inability to keep the scapula glued to the chest, which is much clearer when adding weight (right) 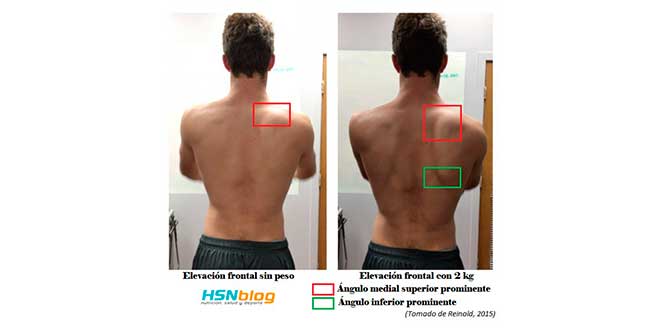
Looking back at the arrows in the first image of the article, the absence of external winging in the right scapula indicates the serratus anterior isn’t properly activated, something very common in training rooms and throwing sports.
Shoulder correction and rehabilitation
It’s true that you should first check for a possible injury to the brachial plexus, but if that’s not the case, you should aim to increase ROM, flexibility, and strength of the weakened muscles.
- Shoulder instability recovery
- 7 Exercise modifications for sore shoulders
Shoulder Impingement
Subacromial syndrome is the most common ailment of the shoulder joint complex
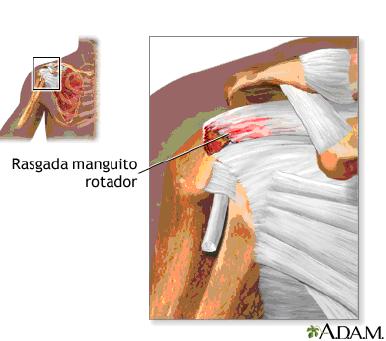
It’s defined as the irritation and inflammation of the tendons forming the rotator cuff as they pass under the coracoacromial arch, as well as bursitis syndrome of the lateral bursa.
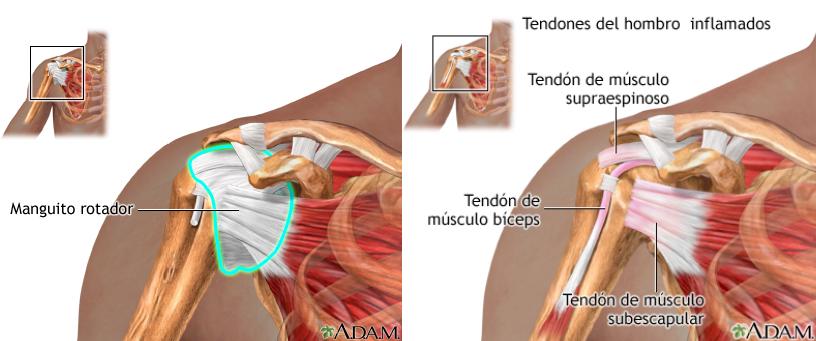
Inside this arch, we find the rotator cuff and the long head of the biceps:
Rotator cuff
It’s made up of the tendons of four muscles: subscapularis, supraspinatus, infraspinatus, and teres minor.
The rotator cuff’s job is to counteract the deltoid’s upward pull on the humerus, stabilizing the shoulder joint. During the first 60º of flexion, this force couple rotates the humeral head. The rotator cuff also performs flexion and external rotation.
Long head of the biceps
The tendon of the long head of the biceps inserts into the supraglenoid tubercle of the scapula.
It passes between the supraspinatus and subscapularis muscles. The long biceps tendon should be functionally considered part of the rotator cuff.
Causes of Shoulder Impingement
- Vascular compressions
- Mechanical factors: Neer showed that during shoulder abduction, the rotator cuff rubs against the anteroinferior third of the acromion. Thickening of the subacromial bursa is also a trigger for friction of the structures passing under the coracoacromial arch.
- Degenerative changes: Degenerative changes in the cuff occur after 50 years of age, worsened by friction against the acromion.
- Traumatic causes: Repeated microtraumas cause degeneration and even tears of the cuff. Repetitive overhead movements are common in sports and work. Especially harmful are bench presses done at 90º and upright rows.

Stages of impingement injury
- STAGE 1: edema and inflammation of the supraspinatus tendon. This is a reversible injury with pain in the front and/or side of the shoulder, worse at night. There’s tenderness over the greater tubercle, supraspinatus tendon, and acromion. Pain occurs between 70-120º of abduction.
- STAGE 2: fibrosis and thickening. At this stage, the bursa is thickened, increasing compression on the rotator cuff. On exam, there’s crepitus and limited active and passive mobility.
- STAGE 3: rotator cuff tear. We distinguish between acute and chronic tears. Acute tears result from trauma, falls on the shoulder, or lifting heavy weight. There’s tenderness over the greater tubercle and weakness in flexion and abduction.
Symptoms of Shoulder Impingement
Pain doesn’t come on suddenly, but starts mild and worsens over time, leading to functional impairment and sharp pain.
The pain is dull with a feeling of fatigue, often appearing at night. When tissues rest, inflammation drainage is impaired, increasing pain. It also worsens with excessive movement.
Treatment and rehab exercises for shoulder impingement
- Conservative treatment as first option: rest, cryotherapy, and NSAIDs. Corticosteroids if pain doesn’t improve
- Physiotherapy: Exercises to stretch and strengthen the rotator cuff muscles (see image below), and avoid, among others, lateral raises, upright rows, or bench press at 90º.
- Arthroscopic surgery can remove inflamed tissue and part of the bone over the rotator cuff. Removing bone can relieve pressure on tendons. It’s indicated whenever there’s a significant tear.
Videos to treat Shoulder Pain
PowerExplosive also helps us with two videos offering examples of correction and injury prevention:
Recommendations
Finally, use proprioceptive massages to learn how to control and position weakened muscles, myofascial release near the anterior clavicle, or stretching the scalene muscles, levator scapulae, and pectoralis minor—these are some of the methods to correct scapulohumeral dyskinesis.
Sources
- McClure, P., Tate, A. R., Kareha, S., Irwin, D., & Zlupko, E. (2009). A clinical method for identifying scapular dyskinesis, part 1: reliability. Journal of athletic training, 44(2), 160.
- Reinold, M. (2015). A Simple Test for Scapular Dyskinesis You Must Use.
- Tate, A. R., McClure, P., Kareha, S., Irwin, D., & Barbe, M. F. (2009). A clinical method for identifying scapular dyskinesis, part 2: validity. Journal of athletic training, 44(2), 165.
- Tejedor, R. L. V., Ordoñez, E. G., Rosa, L. F., y Arriaza, R. (2015). Papel de la disfunción escapulotorácica en la afección de la articulación acromioclavicular. Revista Española de Artroscopia y Cirugía Articular, 22(1), 66-71.
- Van der Helm, F. C. (1994). Analysis of the kinematic and dynamic behavior of the shoulder mechanism. Journal of biomechanics, 27(5), 527-550.
- A. Hüter-Becker. La rehabilitación en el deporte. Editorial Paidotribo (Barcelona) (2005).
- Barlow JC, Benjamin BW, Birt P, Hughes CJ. (2002). Shoulder strength and range-of-motion characteristics in bodybuilders. J Strength Cond Res. Aug;16(3):367-72.
- Beason DP, Tucker JJ, Lee CS, Edelstein L, Abboud JA, Soslowsky LJ. (2013). Rat rotator cuff tendon-to-bone healing properties are adversely affected by hypercholesterolemia. J Shoulder Elbow Surg. Nov 29.
- Kolber MJ, Cheatham SW, Salamh PA, Hanney WJ. (2013). Characteristics of Shoulder Impingement in the Recreational Weight-Training Population. J Strength Cond Res. 2013 Sep 25.
- Ronald P. Pfeiffer y Brent C. Mangus. Lesiones deportivas. Editorial Paidotribo (Barcelona) (2007)
Related Posts
- Exercises to strengthen Shoulders
- Top 10 Shoulder Exercises
- Supplements for Joint Health



