




Chances are this isn’t the first time you’ve heard about an athlete getting an injection to play a match, run a race, or fight. That’s because the player has some pain somewhere in their body, and to keep it from bothering them during the event, sports doctors consider the option of “injecting” them if there’s no risk involved, and the athlete makes the final call.
It’s a technique that, when done right, can be beneficial and helpful but, if done improperly by unqualified personnel, it can lead to an even worse injury.
Corticosteroids
The injection involves administering a series of anti-inflammatory drugs derived from corticosteroids, like hydrocortisone, into the affected area. They’re used when the injury doesn’t respond to other treatments, such as enthesopathies, tenosynovitis, arthritis, bursitis, compression syndromes, some muscle strains…
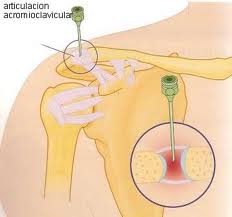
The injections can be intra-articular or extra-articular, and are usually done at the muscle level or around the affected tendon structures (never directly into the tendon due to possible ruptures). The most common is the intra-articular injection of corticosteroid and anesthetic, which reduces inflammation and eases the pain.
Is there a risk? Why doesn’t everyone use it?
Inflammation is a set of biological mechanisms (biochemical and cellular reactions) the body activates in response to various attacks it faces. When injections are used regularly, these mechanisms get altered, reducing pain, yes; but this also means the body takes longer to heal the injury in the medium term, the natural anti-inflammatory response is delayed, and recovery from future injuries becomes less efficient.
Also, cartilage and tendon damage caused by corticosteroids has been reported, so intra-articular corticosteroid injections should be used sparingly, and as mentioned, corticosteroids should never be injected into the tendon body.
Recommendations support no more than 3 or 4 injections per year, with at least 7 days between two injections.
Other methods
On the other hand, less common injections in sports injuries include those with hyaluronic acid or glycosaminoglycans – of debatable effectiveness, although in degenerative processes they seem to protect cartilage by increasing synovial fluid viscosity – and osmotic acid in inflammatory processes and knee effusions, as it somewhat enhances the effects of corticosteroids, though it requires more careful application.
In reality, we need to learn how to regulate inflammation and reduce annoying effects to help tissue repair itself in the best way. In elite sports, this is hard to apply and recommendations often aren’t followed. The weekly event load can be quite high and, remember, it’s the athletes’ job; which often takes priority over their health.
At a recreational level, they should definitely be discouraged.
Sources
- Bahr, R. (2007). Sports injuries: Diagnosis, treatment, and rehabilitation. Madrid. Ed. Médica Panamericana.
- Jiménez Díaz, J.F. (2006). Muscle injuries in sports. International Journal of Sports Science. 3 (2), 45-67.
- Pfeiffer, R. P., & Mangus, B. C. (2007). Sports injuries (2nd ed.). Barcelona. Ed. Paidotribo.
- Sherry, E., & Wilson, S. F. (2002). Oxford manual of sports medicine (Vol. 44). Barcelona. Ed. Paidotribo.



